Former pharma executive Karinza Phoenix is raising $5 million and preparing an ASX listing as Myopharm advances a diabetes drug it hopes can complement the GLP-1 giants.

Karinza Phoenix hasn’t found it hard raising the $6 million that’s got her biotech firm, Myopharm, onto the fast-track approval process for its Type 2 diabetes drug.
“How many times do I present to these high-net-worth individuals and they say, ‘I’m a poorly controlled diabetic’,” Phoenix tells Forbes Australia. “They know what’s coming. Some investors are getting injections weekly into their eyeballs, and they say, ‘We can’t wait for a drug like this, Karinza.”
As pharmaceutical companies scramble to find the next generation of diabetes treatments beyond blockbuster GLP-1 drugs such as Ozempic and Mounjaro, Sydney biotech Myopharm believes it has found a place in the market.
Sydney-based Myopharm’s drug is called TriGlytza and Phoenix is on a pre-IPO roadshow to Singapore, China, Hong Kong and finishing in the US with an American Diabetes Association conference presentation.
Myopharm is seeking $5 million to fund a Phase-2a trial, with an ASX listing pencilled in for the second half of 2026.
Her pitch has resonated with investors, she says, because Myopharm is targeting one of healthcare’s largest and fastest-growing markets with a drug she believes can mop up what’s left after the GLP1 inhibitors like Mounjaro and Ozempic have had their day.
The global diabetes therapeutics market is worth more than US$100 billion annually and is forecast to continue growing as obesity rates rise worldwide. The GLP-1 market is valued between US$62 billion and US$73 billion and is projected to double or triple by 2034.
“75% of people fail their first-line therapy in the first 12 months of being diagnosed with Type 2 diabetes,” Phoenix says. “Eighteen per cent of people fail GLPs. They are GLP naive. We saw an interview with James Packer about that recently. He’s like, ‘it didn’t work for me.’ Some people just don’t get any effect at all.”
TriGlytza has been able to skip Phase 1 safety trials because its three constituent molecules have been well studied in the past. “The FDA put us on a fast-track designation because of all that … and because there’s almost a billion people globally now with diabetes,” says Phoenix.
Professor Mark Cooper, head of diabetes research at Monash University, said the combination of the three existing drugs was a clever idea. He’d worked on one of them, Valsartan, a blood pressure drug, two decades ago.

“They’re using one drug, metformin, which is a classic tablet that you use to reduce sugar. It’s the first drug that’s always used [against Type 2 diabetes], and then they’ve added two other drugs that have been shown to maybe slow the progression of your diabetes … and they’re three relatively cheap drugs.” The other molecule, Celecoxib, is an anti-inflammatory.
Oral TriGlytza could be an effective first line drug, before patients were put on insulin and the more expensive injectables, says Cooper, who is an unpaid advisor to Myopharm.
He said one of TriGlytsa’s constituents, Valsartan, had shown promise for diabetes 20 years ago. “It moderately reduced progression of diabetes but by itself it was not be good enough to be a diabetes drug.” The mechanisms were poorly understood, he said, but inflammation sat at the heart of it.
Mouse studies also held promise that TriGlytza could be used for weight loss, particularly visceral [internal gut] fat, without muscle loss, says Phoenix.
“The problem with a lot of the GLP1 drugs in the market right now is you lose your muscle mass,” she says. “People between 50 and 60 are standing on DEXA scan machines noticing they’ve lost all their muscle, which is a big problem when you’re heading into the years where frailty becomes an issue.”
Phoenix says that TriGlytza will work by treating the root cause of Type 2 diabetes, which she styles as inflammation. “The GLP1s help by getting the weight down, but they don’t always address the underlying disease drivers. And it’s not a one-size-fits-all.”
Towards the patent cliff
The company is betting that combination therapies will become increasingly valuable as large pharmaceutical companies search for replacements for ageing blockbusters. It’s a trend Phoenix knows well.
Phoenix arrived at Myopharm after a career that spanned both big pharma and the capital markets. She joined Novartis fresh out of Auckland University of Technology where she studied animal science and veterinary tech.
She spent two decades inside global pharmaceutical giants including Novartis and Pfizer. When her division at Pfizer was wound down amid regulatory changes in 2015, Phoenix took redundancy and pivoted into investor relations and capital raising.
She spent five years at startup StocksDigital, helping emerging companies navigate IPOs and funding rounds, with a focus on biotechs.
Phoenix and veteran drug developer Dr Milton Grannatt founded Myopharm in 2020, when it was emerging that diabetics were significantly more likely to die from COVID-19 than non diabetics. Evidence was also emerging that diabetes might be causal in a host of other acute diseases, including cancers and heart disease.
They were convinced that despite the rise of new treatments, too many patients were failing to achieve sustained control of the disease.
“Pharma really wants them.”
Karinza Phoenix
“We went around and spoke to biotechnology companies, we spoke to universities, we spoke to the CSIRO, organisations like that. They have IP trade desks, and we got on their registers and worked out what was coming through,” says Phoenix.
Phoenix and Grannatt came across a struggling biotech venture in New Jersey whose founder, Dr Ravi Kumar, had developed a portfolio of patents around a novel treatment for Type 2 diabetes.
Kumar’s Arkay Therapeutics didn’t have the capital to advance it. Convinced of the drug’s potential, Myopharm acquired the TriGlytza IP from Kumar in early 2024 and secured what Phoenix describes as the “golden goose” of biotech development: an Investigational New Drug (IND) approval from the US Food and Drug Administration, allowing the therapy to enter human clinical trials at the phase-2 stage.
“The USFDA don’t let you skip a phase one unless they’re pretty convinced that there’s a lot of data there.”
Myopharm has also extended patent protection out to at least 2046, providing the commercial runway needed to attract a future pharmaceutical partner.
Myopharm will do its Phase 2a study in Australia where generous R&D tax incentives return up to 48 cents in the dollar on eligible expenditure. The study will enrol 48 patients over 16 weeks in a double-blind, placebo-controlled trial designed to assess safety and measure changes in blood glucose control, compared to metformin alone.
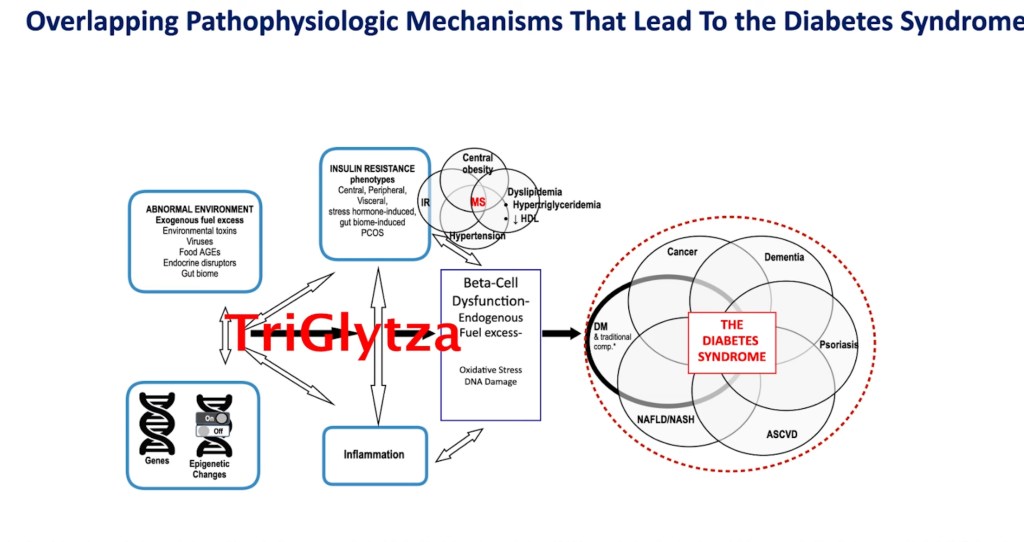
A member of the Myopharm’s scientific advisory panel, emeritus professor of medicine at the University of Pennsylvania, Stanley Schwartz, says inflammation sits at the heart of diabetes. “TriGlytza affects six of the 11 mechanisms of hyperglycaemia: liver muscle adipose tissue, insulin resistance, the gut – because metformin affects absorption of sugar – and obviously, most important, the beta cell.”
Phoenix says the big question that Myopharm hopes to answer is what comes after GLP1s. “There’s obviously mass saturation at the moment,” she says. “Some are coming off patent.
“We are about to experience the worst patent cliff in pharmaceutical history. Thirty-three blockbusters and another hundred drugs will come off patent in the next year. I’ve lived through some pretty big patent cliffs, but this is the biggest one I’ve seen.
“So pharma are desperate to acquire diabetes drugs at that phase-2-trial stage or an IND stage. And we have all those US approvals, so we’re in a really good space. We could be acquired as an adjunct therapy, used with GLP1s. We see ourselves as very much complementary to that space, or we could be used as a monotherapy for Type 2 diabetes.”
TriGlytza is part of a growing class of medicines known as fixed-dose combinations (FDCs), which bundle multiple therapies into a single treatment. Phoenix says the approach has become one of the hottest areas in diabetes drug development, with around 18 FDCs currently progressing through clinical trials globally.
The trend has attracted the attention of major pharmaceutical companies, many of which are looking to complement their existing blockbuster GLP-1 portfolios with combination therapies.
“Pharma really wants them,” says Phoenix. “You’re seeing a lot of the big players moving into the FDC space and acquiring these assets in Phase 2.”
If Myopharm’s Phase 2 trial is a success, it would need a final registration trial looking at about 350 participants over six months.
Phoenix says the company’s preference would be to strike a commercial deal with a pharmaceutical partner before commencing Phase 3, which would need to be conducted in the United States.
Phoenix says Myopharm’s future lies offshore in some form. “We would get 12 emails a night from the US. We’ve already had early-stage interest from GLP companies between the US and Korea. So we will need to be there.”
Want to see more Forbes articles on your feed? Tap here to make Forbes Australia a preferred source on Google.
Look back on the week that was with hand-picked articles from Australia and around the world. Sign up to the Forbes Australia newsletter here or become a member here.